| 2018 submissions will be posted soon | ||
| (click image to view larger version) | Presented at: SAWC Spring: April 2018, Charlotte, NC | |
 |
"Negative Pressure Wound Therapy and Ostomy Accessories Used in Treating Fournier’s Gangrene at a Tertiary Care Center"Richard Schneider, MBA, RN, CWON; Jason Adams, MS, QI System Admin and Reporting Analyst |
|
Abstracts (WOCN® Conference, May 2017)
Wound—Product Selection and Innovations
CS02
INSTILLATION THERAPY AND ITS EFFECTS ON WOUND HEALING
Deanna Zaganas, BSN, RN, WOC, , and Dana Balassa, BSN, RN, WOC, , Glen Burnie, MD
FACILITY: An acute care hospital in the Northeastern United States. CLINICAL PROBLEM: Equipment was available at our facility, but it was not being utilized. We wanted to see if using the instillation* therapy would make a difference in our patient's wound healing. CLINICAL APPROACH: First, it was necessary to get the approval of a few surgeons who would allow us to use instillation* therapy on their patients. After the surgeons agreed on its use on their patients, the inpatient nursing staff had to be educated on how to monitor and/or troubleshoot the instillation* treatment process while they were taking care of a patient receiving this instillation* therapy. Three patients were selected for this case study, and serial pictures were taken at different intervals of their treatment. OUTCOME: The surgeons were happy with the appearance of their patients' wounds when the therapy dressings were changed. The instillation* therapy jump-started the healing process and therefore made the patients happier. The instillation and dwelling of approved fluids avoided the need for the patient to return to the operating room (OR) for washouts with dressing changes. CONCLUSION: Instillation* therapy was effective in jump-starting the wound-healing process and successfully promoted faster healing time while in an inpatient setting. It reduced the surgical risks to these patients by avoiding the need to return to the OR under anesthesia.
http://http://www.acelity.com/products/tech/vera-flo-therapy. Published 2014.
http://http://www.acelity.com/products/vac-veraflo-dressings. Published 2014.
http://http://www.veraflo.com/about-v-a-c-veraflo-therapy. Published 2016.
Kim P, Attinger C, Crist B. Negative pressure wound therapy with installation: review of evidence and recommendations. Wounds. 2015;27(12):1–20.
Kim P, Attinger C, Steinberg J, et al The impact of negative pressure wound therapy with instillation compared with standard negative-pressure wound therapy: a retrospective, historical, cohort, controlled study. Plast Reconstr Surg. 2014;133:709–716. View Full Text | PubMed | CrossRef
Wound—Product Selection and Innovations
CS05
A SWEET SOLUTION: THE USE OF MEDICAL-GRADE HONEY ON ORAL MUCOSITIS IN THE PEDIATRIC ONCOLOGY PATIENT
Ferne Elsass, MSN, RN, CPN, CWON, , Norfolk, VA
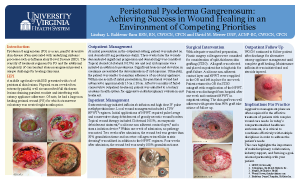
PROBLEM: Pediatric patients develop mucositis when receiving treatments such as chemotherapy and radiation. The gastrointestinal mucosa's epithelial cells divide quickly, leading to breakdown and painful ulceration. The most common and sensitive is oral mucositis. Patients developed painful bleeding ulceration and thick mucoid saliva. Lips eventually crack and bleed. Mouth rinses containing antimicrobial, antihistamine, and analgesic medications are the mainstay for pediatric patients. These rinses are often refused related to taste or texture. Patients less than a year old are unable to use these products. Continued oral mucositis leads to increased pain and refusal or inability to eat. PROJECT OBJECTIVE: Outcomes from oral mucositis such as decreases in nutritional intake and deteriorating oral hygiene developed from the painful, bleeding ulcers and dry crusting of the mouth. Alternatives to standard treatments were necessary. Leptospermum honey was added to daily mouth care. At completion of this poster, this treatment has been used in 10 pediatric oncology patients between the ages of 9 months and 17 years. CASE SERIES: To demonstrate the improvement of oral mucositis with standard oral care and the additional use of active Leptospermum honey in 3 pediatric oncology patients. OUTCOME: The Leptospermum honey paste was easy to apply and well received by all patients. The patient received oral care every 4 hours, followed by the application of the honey paste 2 to 3 times daily. The paste was applied with a sponge swab, coating the mouth. Patients either swished and spit or had excess suctioned out. Three selected examples of the 10 patients are presented in the poster. Leptospermum honey paste proved to be effective in all participating patients. Healing observed within 3 days, and patients in all cases reported decreases in pain. Decrease in wounds and bleeding was evident in all cases within 5 days.
1. Miller M, Donald D, Hagemann T. Prevention, treatment of oral mucositis in children with cancer. J Pediatr Pharmacol Ther. 2012;17(4):340–350. PubMed
2. Molan P, Rhodes T. Honey: a biologic wound dressing. Wounds. 2015;27(6):141–151. PubMed
3. Rashad U, Al-Gezawy S, El-Gezawy E, Azzaz A. Honey as topical prophylaxis against radiochemotherapy-induced mucositis in head and neck cancer. J Laryngol Otol. 2009;123:223–228. doi:10.1017/S0022215108002478. PubMed | CrossRef
4. Song J, Twumasi-Ankrah P, Salcido R. Systematic review and meta-analysis on the use of honey to protect from the effects of radiation-induced oral mucositis. Adv Wound Care. 2012;25(1):23–28.
Professional Practice—Restructuring in Health Care Settings, Strategies for Survival
PI08
A JOURNEY OF EXCELLENCE: ACHIEVING THE JOINT COMMISSION DISEASE-SPECIFIC CARE CERTIFICATION IN WOUND CARE
Ann Roberts, BSN, RN, PCCN, , Tara Beuscher, DNP, RN-BC, GCNS-BC, ANP-BC, CWOCN, CFCN, , Melissa Parker, RN, CWOCN, , Elizabeth Longwell, BSN, RN, CWOCN, , and Julie McAuley-Gonzalez, BSN, RN, CWOCN, , Transitional Care, Charlottesville, VA
On opening 6 years ago, it quickly became apparent that this long-term acute care hospital would be a home for management of many patients with complex wound issues that accompanied their multiple other medical diagnoses. The patient population at this hospital presented a challenge that was unique. Certified wound ostomy continence nurses (CWOCNs) and the interdisciplinary team have worked to develop and implement a wound care program that provides an interdisciplinary and evidence-based approach to wound care including the training of close to 40 clinicians from the interdisciplinary team in a nationally recognized Wound Treatment Associate Program. This poster presentation traces the evolution of wound care services at this hospital through the process of active application for Disease-Specific Care Certification in Wound Care. It outlines and makes accessible to its audience The Joint Commission requirements for Disease-Specific Care Certification.
Horn J. One program's journey to Joint Commission certification for wound services. J Acute Care Phys Ther. 2012;3(3):242–245.
Isbey C, Roberts W. Disease-Specific Care Certification most cited standards: reviewers' insight [webinar]. https://attendee.gotowebinar.com/recording/3916492673968054018?source=website-doc. Published October 19, 2015.
Morrison K. The road to JCAHO disease-specific care certification: a step-by-step process log. Dimens Crit Care Nurs. 2005;24(5):221–227. View Full Text | PubMed | CrossRef
The Joint Commission. Certification Review Process Guide. Oakbrook Terrace, IL: The Joint Commission; 2012.
The Joint Commission. Benefits of Joint Commission certification. http://http://www.jointcommission.org/benefits_of_joint_commission_certification. Published 2015.
Wound—Preventative Practices New
PI11
IMPLEMENTATION OF A COST-EFFECTIVE PRACTICE FOR REDUCING BOTH PRESSURE INJURY AND HEALTHCARE WORKER INJURY DURING PATIENT REPOSITIONING
Deanna Zaganas, BSN, RN, WOC, , and Dana Balassa, BSN, RN, WOC, , Glen Burnie, MD
BACKGROUND: Nurses have more injuries than any other occupation, with the majority of injuries occurring during patient handling. Recent data support that in-bed repositioning is a significant source of risk for healthcare worker injury (HCWI). These injuries are estimated to cost $22,500 each, adding $750 million in annual cost to US healthcare. Patient care standards for pressure injury (PI) prevention require acute care nurses to reposition patients in the bed as often as 6 to 10 times per shift, a significant source of HCWI risk. The goal of our project was to (1) decrease HCWI during in-bed repositioning and (2) prevent hospital-acquired sacra/buttock PI (SBPI). METHODS: We implemented a new patient positioning system (PPS) designed to (1) decrease the nursing effort required for in-bed repositioning and (2) off-load the sacrum and buttocks for PI prevention. The new practice included the use of the PPS for all patients requiring assistance with in-bed mobility. We compared outcomes before/after implementation, estimated the increase in our annual PPS spend and cost avoidance from expected decreases in HCWI/SBPI, and calculated our annual return on investment (ROI). RESULTS: Comparison of preimplementation (2015) to postimplementation (2016) found decreases in both SBPI (10.6 to 6.3 per month) and HCWI. Based on annual admissions, we expected 13 patients per day (25%) to use the PPS and found our actual use at 11 patients per day. Product spend was $677,272 and cost avoidance was $861,000, providing an annual ROI of $183,728. CONCLUSION: With the Centers for Medicare & Medicaid Services' trend toward value-based purchasing that links healthcare quality to payments, hospitals have become increasingly focused on quality. Overall quality is composed of both cost of care and realized outcomes. When cost avoidance from improved outcomes exceeds the cost of care, there is improved quality value for both patients and hospitals.
Fragala G, Boynton T, Conti MT, et al Patient-handling injuries: risk factors and risk-reduction strategies. Am Nurse Today. 2016;11(5):40–44.
US Department of Labor, Bureau of Labor Statistics. Nonfatal occupational injuries and illnesses requiring days away from work, 2009. http://http://www.bls.gov/news.release/archives/osh2_11092010.pdf. Published 2010.
Occupational Safety and Health Administration. Guidelines for Nursing Homes: Ergonomics for the Prevention of Musculoskeletal Disorders. Washington, DC: Occupational Safety and Health Administration; 2009.
Wound—Preventative Practices New
PI23
DRIVING DOWN TRACH-RELATED PRESSURE INJURIES
Margaret Hiler, MSN, RN, CWOCN, , Nursing Administration, Washington, DC; Dot Goodman, BSN, RN, CWOCN, , Gerogetown University Hospital, Washington, DC; Ashna Saxena, MHA, , Utilization-Quality Improvement, Washington, DC; and Jenna Riley, BSN, RN, CCRN, , Washington, DC
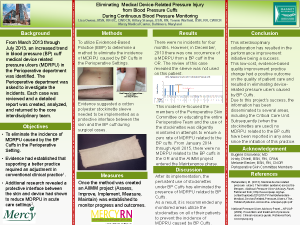
PROBLEM: Development of pressure injuries underneath medical devices is becoming increasingly prevalent in critically ill patients.1 In one acute care academic medical center in the mid-Atlantic region, 40% to 45% of all pressure injuries are related to medical devices. Many pressure injuries develop underneath the faceplate of tracheostomy tubes in patients in an intensive care unit (ICU) who underwent an emergent or bedside tracheostomy. Nurses attribute injuries to lack of pressure-relieving dressing usage. Dressing usage is often limited by tight suturing and unclear communication between nurses and pulmonary physicians, resulting in delayed suture removal. OBJECTIVES: To decrease trach-related pressure injuries (TRPIs) by: • identifying a dressing that effectively reduces pressure, moisture, and contact between skin and trach faceplate; • improving communication between physicians and nurses. METHODS: A group of key ICU stakeholders including nursing, physicians, and a WOC nurse convened and identified areas for improvement: (1) the available moisture-wicking dressing was disliked by physicians and therefore not being used; (2) standardization of trach care in this population. OUTCOMES: • The WOC nurse acquired samples of several products. Physicians and nurses identified a highly absorbent polyurethane tracheostomy dressing as the preference for use at time of insertion and for continued care. • A clinical nurse III developed a communication form to be placed at patient's head of bed to display pertinent care protocols and lines of communication. RESULTS: In the fiscal year (FY) 2015, there were 8 TRPIs. There were also 8 TRPIs within the first 2 quarters of FY2016. Upon implementation of the aforementioned interventions, there was 1 TRPI in quarter 1 (Q1) and zero in quarter 2 of FY2016. There was 1 TRPI in Q1 of FY2017. Audits of use of bedside communication tool showed 100% compliance.
1. NDNQI. Pressure ulcer training v. 5.0. https://members.nursingquality.org/NDNQIPressureUlcerTraining/module1/MDRPressureUlcers.aspx. Published 2016. Accessed November 1, 2016. Cited Here...
Continence—Issues in Bladder and Bowel Continence Management
PI40
CHANGE IN PRACTICE TO DECREASE USE OF INTERNAL FECAL MANAGEMENT SYSTEM
Jeanne Arseneau, MSN, RN, CWOCN, , Wound, Ostomy & Continence Department, Rosedale, MD
Fecal incontinence with diarrhea in the acute care setting requires careful and attentive management to prevent skin breakdown and infection. The use of an internal fecal management system (IFMS) diverts liquid or semiliquid stool into a collection bag, but it has potential risks of causing serious patient harm. At a community hospital in the Northeast, it was discovered that the IFMS was used very frequently, the documentation system did not include a section for the IFMS, and the hospital policy needed updating and clarification for the role of the nurse and the medical staff. During the process of developing the new documentation and policy update, a safety alert was received from our Corporate division concerning 2 rectal perforations in a sister hospital. The safety alert accelerated the completion of the new documentation and the policy. Education was disseminated to the nursing and medical staff on the new policy regarding indications, contraindications, medication reconciliation, use of fecal pouch prior to considering the IFMS, medical staff assessment of anal sphincter tone, and guidelines for discontinuation. The new change in practice resulted in decreasing the IFMS usage from 391 to 122 and cost savings of $43,000 for the year.
Guidelines for the management of fecal incontinence with Flex-Seal SIGNAL Fecal Management System (FMS). http://http://www.convatec.com/media/4431973/guidelines ap-012616-us.pdf. Accessed May 15, 2015.
Mulhall AM, Jindal SK. Massive gastrointestinal hemorrhage as a complication of the Flexi-Seal fecal management system. Am J Crit Care. 2013;22(6):537–543. View Full Text | PubMed | CrossRef
Wilson MM, Angyus M, Beals D, et al Executive summary: a quick reference guide for managing fecal incontinence (FI). J Wound Ostomy Continence Nurs. 2014;41(1):61–69. View Full Text | PubMed | CrossRef
Posters
| (click image to view larger version) | Presented at: | |
 |
WOCN® Conference: June 2016, Montreal, Cananda | |
 |
WOCN® Conference: June 2016, Montreal, Cananda | |
 |
WOCN® Conference: June 2016, Montreal, Cananda | |
 |
2016 MAR Conference |
|
 |
October 2015 SAWC conference in Las Vegas |
|
 |
Maryland Organization for Nurse Leaders (MONL) and MAR Conference, Richmond, VA - Summer, 2016
|
|
 |
WOCN® Conference: June 2016, Montreal, Cananda
|
|
See our Posters Archive page for more
To have your poster shown here, please send a PDF file of your poster, along with information you would like to show to:
webmaster@marwocn.org.
![]()